Anatomy and surgery; inseparably linked
Prof Dr Theo Wiggers · · 9 min readA doctor in training for a surgical discipline may only perform surgery on a patient once they have attained a sound understanding of a procedure followed by practical exercises in a skills center.
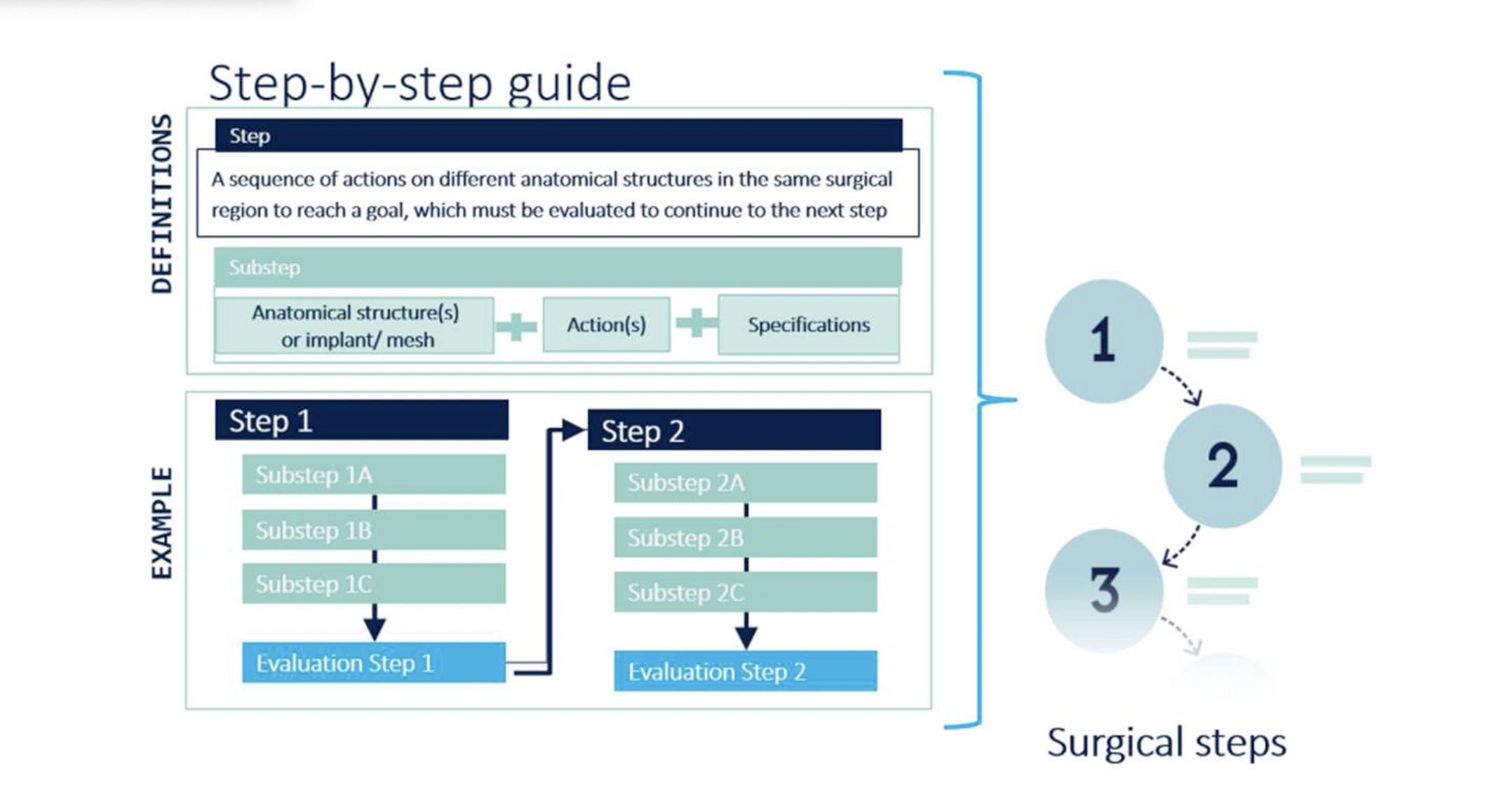
To avoid cognitive overload while learning surgery, it is wise to break down each operation into a series of steps. Steps can, in turn, be broken down into several substeps. Substeps are based on anatomical structures and on a few occasions on implants [2]. This anatomical structure then is involved in an action (Figure 1). This is a verb that describes what type of action is carried out by the surgeon on which specific anatomical structure. Each verb has an unambiguous definition. Examples of the verbs are: incise (the skin), ligate (the vessel), transect (the duct). Knowledge of anatomy is therefore a prerequisite for learning, performing, and evaluating a procedure.
Anatomy: an important part of knowledge for surgery
The foundations of the anatomical knowledge are laid at the beginning of the medical study. Anatomy remains an important part of the knowledge of operations throughout training as a specialist. Even after that, surgeons will need anatomical knowledge time and time again if they wish to adopt a new procedure or a variant of an existing procedure. Each time also for the experienced surgeon the process restarts with a step-by-step description of the operation. Even then, in each substep, an anatomical structure as object of the verb describing the action, shall be named. The extensiveness and detailing of anatomical knowledge are not the same during the study and training and will have to fit in the phase of study or training the student/resident has reached. From broad and global to specific and detailed. The building of knowledge must be done through a logical plan and preferably take place in one learning environment.
Learning by region to build student's knowledge effectively
Students start learning the anatomy of regions [2]. For example, the lower leg. This knowledge should be integral. Bones, muscles, nerves, blood vessels, lymph node stations and fascia are learned in coherence. To gain a good understanding, regions must have a certain size. Only then can you see and understand origo and insertion and with it the whole course of a muscle or the branching course of nerves and blood vessels. As soon as the student knows the topography of the structures, the functional anatomy is added to it. Then it becomes clear how, controlled by the nerves by muscle action on joints, the bones and thus the extremities, head/neck, back or abdominal wall can move. Learning is facilitated if the knowledge is offered in 3D and interactive. A 3D anatomical model with selective turning off and naming of certain structures is helpful. The most intensive way of studying is a model of the human body projected into virtual reality environment with interactive questions [3]. In the best virtual models, the movements are also integrated. The student's knowledge is thus built up by region and is also causally linked to physiology and later pathophysiology. Finally, the pathological anatomy will be added during the study. Under the influence of diseases (inflammation or tumors) or by anatomical variations are the position, relationship to the surrounding structures and the function of anatomical structures affected. This way, the content is going to live for the student. However, the anatomical knowledge of the regions should remain global and not be elaborated in detail. For example, the approach of an anatomical structure via a skin incision or endoscopy will not be necessary knowledge at that stage of the study.
The anatomy challenge for interns
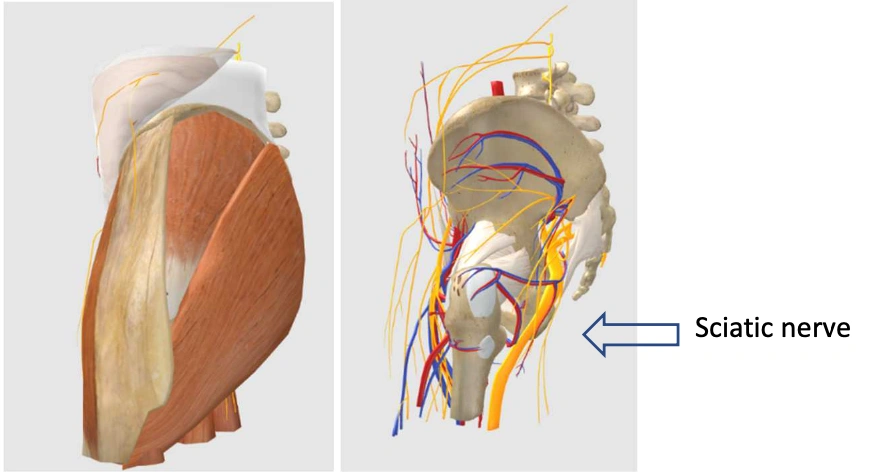
For the intern, this will be different during the surgical internships. During the preparation for an operation, the anatomical knowledge is used in a different way. Some structures that were clearly visible when studying the regional anatomy do not appear in a specific procedure in vision. The same model that was used during the bachelor phase can now in a similar manner be used to remove layers of skin and muscles and subsequently see the relationship from the nerve to the bone. For example, in a hip operation, the sciatic nerve will be visible in the operation field directly, but it is important for a resident to know the distance to the nerve when approaching the femoral head (figure 2).
Procedural anatomical knowledge is needed to understand how the surgeon will achieve his goal step by step through a skin incision or after trocar placement and which anatomical structures should be set aside before the place where the operation is to be performed is visible. An example are the short neck muscles during thyroid surgery. During the anatomy lessons of the student in the bachelor phase these muscles were shown from origin to insertion but during operation only a part is visible and will after dissecting it free and keeping aside part of the muscles the thyroid gland become visible. By keeping the muscles aside, the image that the student was used to, has now changed in a different anatomical picture. Also, the orientation is different because the viewing angle is not the same as it was when studying the anatomical model. It helps the student in understanding the new situation enormously if the anatomical model can be rotated in 3D towards the viewing direction. The changes that occur by mobilization of structures are difficult to simulate in the original model but can be built into the Virtual Reality environment.
Why the resident in training will need even more detailed knowledge of the anatomy
Now three- dimensional insights are required to understand the position of structures in relation to each other. Not only do the anatomical structures need to be recognized, but also the risks that arise when they are dissected. The changes occurring due to illness in the organ for which the operation is performed must be understood from the direction of view of the operator. With the same thyroid operation, the course of the recurrens relative to the thyroid gland is crucial and certain structures such as the parathyroid glands are not so clearly distinguishable from the thyroid tissue. Finally, there are anatomical variations that need to be known and recognized. In the case of thyroid surgery, a non- recurrent recurrent nerve.
During his training, the resident will differentiate in a subspecialty or choose for another surgical discipline. The general knowledge of anatomy will decrease, but the knowledge needed to operate in this specialty will only increase. Detail knowledge of skin nerves or the autonomic nerve system will then become important to cause as little damage as possible during surgery. Any change in anatomy caused by illness, patient, or congenital variations (e.g., malrotations of the intestines or aberrant kidney arteries) must be known. Functional recovery or recovery from complications also requires insight into the anatomy. For the experienced surgeon who wants to develop a new procedure, it will start again with a step-by-step description based on anatomical structures. After that, the procedure will be practiced on human bodies before the first patient is treated. Besides proctoring (structured 4 supervision) learning with the aid of videos is important [4].
Mastering anatomy takes time
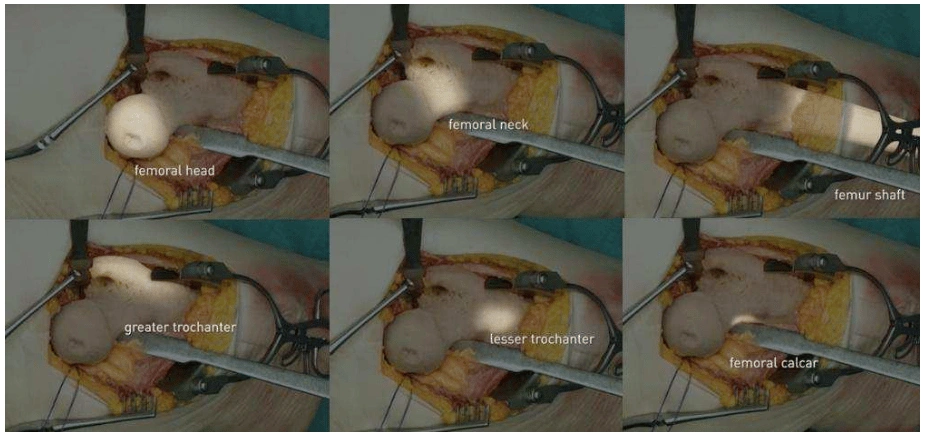
Gaining and maintaining knowledge and skills are a life-long process. Sometimes by learning new interventions but usually by retrieving and deepening existing knowledge around an operation. It is of advantage if learning the anatomy, functional anatomy and the procedural anatomy occurs in one integrated learning environment. All anatomical structures are linked to anatomical terms with the corresponding definitions. Each time it can be built on the preceding. In the Incision Academy the we are aware of this. The modules of regional anatomy are available in 3D supplemented with interactive learning in virtual reality. It also includes examples of joint movements with the aim of learning functional anatomy. For the procedural anatomy, the basis is laid in the step-by-step description of an operation in combination with a video film with highlights (figure 3).
This procedural anatomy is now being made interactive and will soon be available in virtual reality for 50 procedures.
In summary
In summary, for a doctor who does surgery anatomy is one of the most important pillars of the work. The student will need to know the structures in their mutual relation, the intern the first procedural knowledge and the doctor in training three-dimensional insight of structures that come into a different position by the surgical intervention or the disease of the organ.
Ready to start learning?
Explore a wide variety of anatomy courses and 3D models on the Incision Academy. The Academy includes over 500 high-quality video courses on surgical procedures to prepare for your work. Explore surgical procedures step by step in 2D & 3D, master basic principles and skills, anatomy, medical technology, and much more. We bring together everything that’s required to optimize OR performance.
[1] Nazari T, Vlieger EJ, Dankbaar MEW, van Merriënboer JJG, Lange JF, Wiggers T. Creation of a universal language for surgical procedures using the step-by-step framework. BJS Open. 2018; 2:151-157.
[2] Smith CF, Finn GM, Stewart J, McHanwell S. Anatomical Society core regional anatomy syllabus for undergraduate medicine: the Delphi process. J Anat. 2016; 228:2-14.
[3] Zhao J, Xu X, Jiang H, Ding Y. The effectiveness of virtual reality-based technology on anatomy teaching: a meta-analysis of randomized controlled studies. BMC Med Educ. 2020; 20:127.
[4] Shim JS, Kim JY, Pyun JH, Cho S, Oh MM, Kang SH, Lee JG, Kim JJ, Cheon J, Kang SG. Comparison of effective teaching methods to achieve skill acquisition using a robotic virtual reality simulator: Expert proctoring versus an educational video versus independent training. Medicine (Baltimore) 2018; 97:51(e13569).







